
III. Patient Selection and Preparation
A. Patient Assessment: How will I know the patient is suitable for moderate sedation administration?
Each patient receiving moderate sedation must have a physician/LIP assessment completed within 30 days prior to the procedure AND updated on the day of the procedure. (In an emergency situation, these requirements may be waived.) Elements of the assessment must include:
1. History and Physical including:
a. Significant medical/surgical history
b. Significant family history
c. Smoking history
d. Alcohol/drug abuse
e. Possible pregnancy (LMP)
f. Airway risk history *
g. Physical exam of heart and circulatory system
h. Physical exam of lungs
i. Physical exam of airway **
j. Level of consciousness/mental status
k. Review of current medications
l. Allergies/previous adverse drug reactions
m. Pertinent lab or test results
* Risk factors and physical findings associated with a difficult airway management include:
- History of previous complications, sleep apnea, stridor, snoring, neck arthritis
- Hoarse voice or previous tracheostomy could indicate possible stenosis at some level
- Significant obesity (especially involving the neck and facial structures)
- Head and Neck: Short neck, limited neck extension
- Neck examination: check for masses, mobility, deviation of the trachea.
- Mouth: small opening (<3 cm in an adult), edentulousness, presence of a beard, loose or capped teeth, high arched palate, tonsillar hypertrophy, non-visible uvula, temporomandibular joint problems.
- Mouth examination: an opening of at least two large finger breadths between the upper and lower incisors in the adult is desirable.
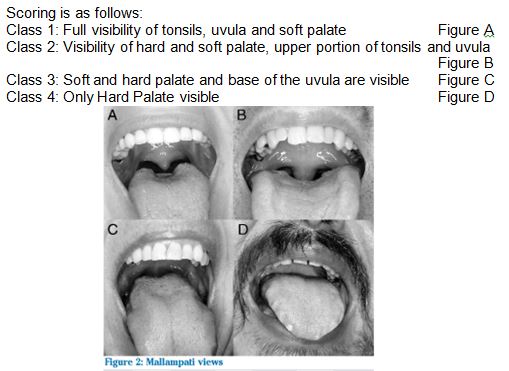
** Physical examination of the airway may include the Mallampati classification. In anesthesiology, the Mallampati score, also Mallampati classification, is used to predict the ease of intubation. It is determined by looking at the anatomy of the oral cavity; specifically, it is based on the visibility of the base of uvula, faucial pillars (the arches in front of and behind the tonsils) and soft palate. Scoring may be done with or without phonation. Higher Mallampati Score (Class 4) is associated with more difficult intubation as well as a higher incidence of sleep apnea.
2. The American Society of Anesthesiology (ASA) Physical Status Classification system (ASA Classification) will be employed in determining the suitability of the patient for moderate sedation administration. The physician/LIP performing the moderate sedation will be responsible for the assigning and documentation of the patient's ASA class.
Review of ASA Physical Status Classification System:
Class I: A normal healthy patient
Class II: A normal patient with mild systemic disease
Class III: A patient with a severe systemic disease that limits activity but is not incapacitating
Class IV: A patient with an incapacitating systemic disease that is a constant threat to life
Class V: A moribund patient not expected to survive 24 hours with or without the procedure
Most patients in Class I-III will generally tolerate minimal and moderate sedation without any problems. However, use of moderate sedation for patients in Class IV and V is of higher risk.
3. Informed Consent The Physician/LIP performing the procedure must inform the patient/guardian about the risks, benefits and alternatives to sedation as a component of the planned procedure. The Physician/LIP prior to the procedure must document this discussion in the medical record with date and time. This requirement does not apply to emergencies.
4. Patient education: Age-appropriate patient education should be provided to all competent patients and/or their family member, answering any questions prior to the administration of sedation. Psychological preparation of the patient is always important. Thorough preparation can contribute to sedation that is more effective and may even reduce the need for higher doses during the procedure.
5. Transportation Arrangements
An arrangement for transportation home with an individual who accepts responsibility is to be determined before the patient is sedated. Without these satisfactory arrangements, the physician ordering the sedation or performing the procedure must be notified in advance of this situation. The Physician/LIP will then determine if the administration of sedation will proceed as planned and document medical necessity to proceed as planned.
Pediatric patients: When moderate sedation is used for a pediatric patient, a qualified physician/LIP or an anesthesia provider must be present at bedside to sedate the patient.
B. Reassessment: What must be done immediately before the administration of moderate sedation?
1. Physician/LIP Reassessment: must be performed immediately prior to the moderate sedation to assure that the patient remains a candidate for the planned sedation. Evaluation will include a review of the patient’s Pre-Sedation Assessment (H &P) to confirm there have been no changes. (In an emergency situation, this requirement may be waived.)
2. Nothing By Mouth (NPO) status must also be considered when performing moderate sedation as patients will be at greater risk of aspiration if they become over-sedated. Patients at risk for aspiration include: morbidly obese patients, patients with history of reflux esophagitis, hiatal hernia, pregnant patients in their last trimester of pregnancy, full stomach patients. (In an emergency situation, this requirement may be waived.)
NPO status (time and nature of last oral intake)
a. Minimum fasting period: 2 hours (clear liquids)
b. Minimum fasting period: 6 hours (light meal)
c. Minimum fasting period: 8 hours (heavy meal)
d. Exceptions to fasting include sips of water for swallowing medications, required oral preparations and per physician discretion
3. Time Out: Time out and site marking must be performed and documented according to the Universal Protocol for Prevention and Wrong Site Wrong Surgery (system policy).