
VI. Complications
Under ideal circumstances, the patient undergoing a procedure under “moderate sedation” is able to experience a pain free procedure with minimal risk. However, deeper levels of sedation are sometimes required to accomplish the goal of painlessness, and higher doses of more potent medications must be utilized. This puts the patient at higher risk of medication side effects, hemodynamic instability, loss of protective reflexes including airway control, hypoxia, and cardiac arrhythmias.
The Physician/LIP in charge of the procedure must have a working knowledge of the common reasons for patient instability in this setting, and the tools necessary to regain control of the situation.
While this section will deal with arrhythmia interpretation and use of common medications, it is vital to always first assess the “ABC’s” before other interventions. Very commonly, the reason for an arrhythmia or drop in blood pressure often regains stability without requiring medication. The goal of this section will be to obtain a working knowledge of some basic arrhythmias, and some medications that may be useful in the first few minutes of a patient decompensating.
A. ABC: First and foremost is to systematically evaluate the patient in distress. In Emergency Medicine, the initial evaluation of an unstable patient follows the “ABC’s.”
Airway
Protective reflexes may become absent. Maintain the airway by chin lift or jaw thrust technique and/or insert a nasal or oropharyngeal airway, if appropriate, to assure the tongue does not occlude the airway. Suction as necessary to maintain a patent airway. If apnea or airway obstruction is not properly treated, they may result in cardiac arrest.
If Airway obstruction occurs, the following sedation airway management algorithm should be followed
1. Head tilt
2. Chin lift
3. Jaw thrust and consider pharmacologic reversal
4. Call for additional assistance
5. Insert oral airway
6. Attempt Positive pressure Ventilation (Ambu bag)
7. Call Respiratory Prepare for intubation
(Adapted from Moderate sedation/analgesia, 2nd edition, Kost, 2004)
Head Tilt: Moves the head from the neutral position to the lateral (side) position. This maneuver may result in tongue displacement from the posterior pharyngeal wall to the side of the oropharnyx
Chin Lift: combined with hyperextension of the head and neck and forward displacement of the mandible will elevate the soft tissue anteriorly and open the airway.
Jaw Thrust: If tactile stimulation, head tilt, and chin lift do not produce relief of airway obstruction, attempt the jaw thrust. The jaw thrust maneuver places significant anterior forward displacement on the jaw in an attempt to relieve obstruction and restore air flow. Great care must be taken not to exert excessive pressure for a prolonged period of time when performing a jaw thrust to prevent damage to the facial nerve.
Breathing
The most serious effect of many of the moderate sedation agents is respiratory depression, which can progress to apnea, even in arousable, responsive patients. Apnea must be immediately treated by assisting ventilation with a bag valve mask with reservoir and 100% supplemental oxygen.
Circulation
Hypotension should be treated by placing the patient in the modified Trendelenburg position. An intravenous fluid challenge, and/or vasopressors may be used at the direction of the physician. The appropriate reversal agent(s) should be drawn up and readied for administration. If ECG rhythm disturbances occur, the physician is responsible for ordering appropriate treatment can be obtained. Be sure to obtain a strip and attach it to the documentation forms.
B. Cardiac Rhythm Identification
The following will be a review of common arrhythmias and a methodology for identification. Once again, it must be stressed that the first step in assessing a patient with an abnormal monitor tracing is to assure adequate airway, breathing, and circulation. If the patient has a good blood pressure, then the rhythm is “stable” and definite treatment need not be initiated emergently. Identifying a rhythm off a monitor tracing is often difficult. Make sure the leads are making good contact with the patient, and print out a rhythm strip to analyze.
Rate: Bradycardic < 60
Tachycardic > 100
Is it a sinus rhythm? If there are P waves associated with every QRS complex and the PR interval is consistent then the rhythm is sinus.
If the rate is bradycardic, is there a heart block? Are there more P waves than QRS complexes present? In a complete heart block (3rd degree block) the P waves do not conduct, and there is no relationship between the P waves and the QRS complexes.
In a 2nd degree block some of the P waves conduct, but there will be some P waves without a QRS (“dropped beat”).
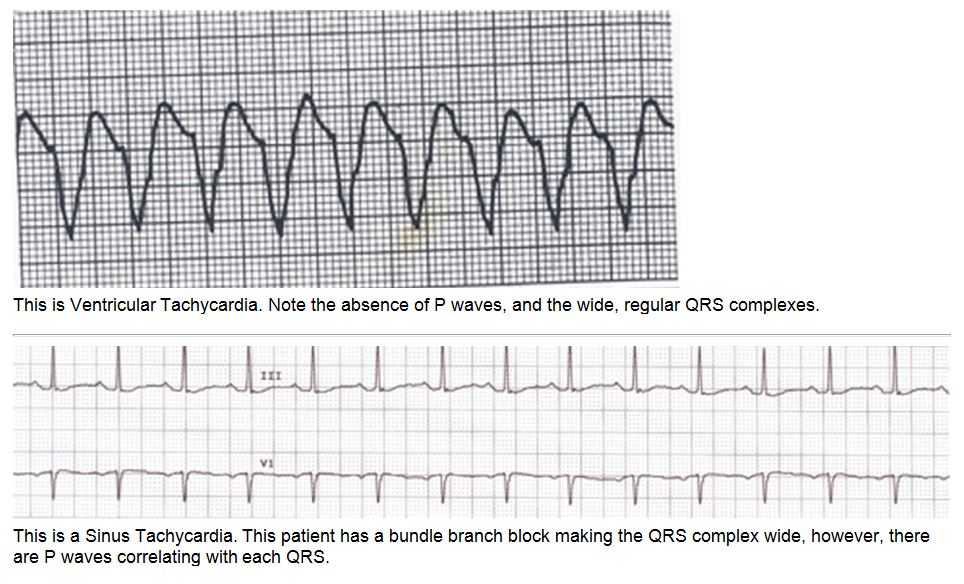
If the rate is tachycardic and not sinus, then the first question is whether the QRS complexes are narrow or wide. This can often be quite difficult to ascertain depending on the rate. “Classic” Ventricular Tachycardia (Vtach) has a sine-wave appearance, with wide complex, regular QRS complexes.




C. Defibrillator Operation:
There are different types of defibrillators available throughout Aurora. Basic operation is quite similar. Every unit has the capability to be used as a monitor, as well as a defibrillator. Attach monitor leads, and set the machine to display the rhythm strip. If in doubt as to the rhythm, the unit can change the lead it is displaying. You also have the option of reading the rhythm through the paddles “quick look.” This is especially helpful for Vtach / Vfib where early defibrillation is essential. You can always continue to monitor the rhythm on a dedicated cardiac monitor, and use the defibrillator to deliver a shock.
Initial defibrillation is only for the unstable patient. Otherwise, calling a code or arranging immediate transfer to the emergency department is preferred.
To defibrillate, first turn the unit on. The patient can be shocked via sticky pads, or hand held paddles. Set the desired energy level. Make sure the paddles or pads are firmly attached. Ideally, one pad is placed to the right of the sternum just below the clavicle, and the other to the left of the nipple in the mid-axillary line. Make sure the area is clear and press the defib button.
The patient can also be paced externally using the defibrillator unit. Pacemaker pads should be placed anteriorly and posteriorly. Start with a moderate rate of 60-80. Slowly increase the current until there is capture.
Cardiopulmonary resuscitation should be initiated if the patient becomes pulseless and/or non breathing.